Northern Utah pain management providers concerned about longtime opioid users

Theodore Viegas talks about the constant pain he lives with Friday, Nov. 17, 2017, at his sister’s home in Farmington. Viegas keeps a box of more than 32 medications to combat his pain and other symptoms from multiple sclerosis.
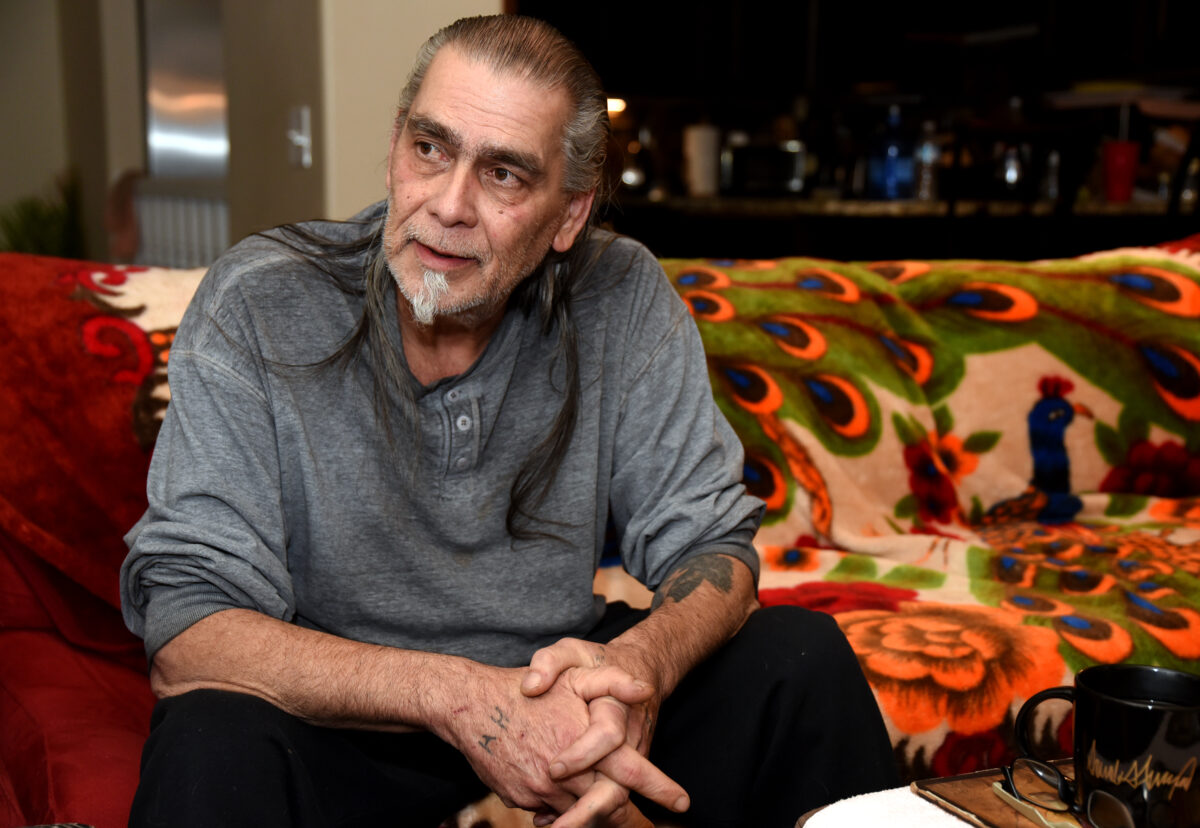
Theodore Viegas talks about the constant pain he lives with Friday, Nov. 17, 2017, at his sister’s home in Farmington. Viegas takes prescribed opioids to deal with the pain from multiple sclerosis. The disease has caused muscles, especially in his legs, to degenerate. “I’m basically walking on bones,” he said.
Theodore Viegas talks about the constant pain he lives with Friday, Nov. 17, 2017, at his sister’s home in Farmington. Viegas keeps a box of more than 32 medications to combat his pain and other symptoms from multiple sclerosis.
KAYSVILLE — Dr. Christian Obah devotes his days to helping chronic pain patients maximize their quality of life. For many, that means weaning them off high doses of opioids by offering alternatives that render some relief.
For almost five years, Obah has been treating patients at Lifespring Pain Management Center in Kaysville. But the nation’s alarming opioid overdose crisis hit Utah in a big way — the state ranked 7th in the U.S. for drug overdose deaths in 2015 — thus ushering in new legislative limits on the amount of narcotics physicians can prescribe. For individuals who have relied on prescription opiates for years or possibly decades, those constraints could be deadly.
“We’re seeing patients from other clinics who are on very high amounts of medications,” Obah said. “And when they don’t get them to treat their pain, they resort to street drugs. To me, that’s even more dangerous. … You don’t know what’s laced in, and it might not be what the patient was hoping to get.”
Opiate medications, in general, can be addictive, Obah added, and part of his job entails teaching patients about their dangers, side effects and consequences.
For Ogden resident Dotti Wilkerson, one of Obah’s patients, her chronic pain dates back to 1973, when a car accident left her with a crushed pelvis, fractured jaw and other problems. The Jaws of Life had to be used to get her out of the vehicle, and at the time, she was four months pregnant with her fourth child. Wilkerson spent five months in traction in the hospital, with morphine intravenously subduing her pain. Her baby survived and was born in 1974.
“I went home on morphine,” Wilkerson said. “I have a very big tolerance for opioids.” But she could function and was thankful to be alive.
“I raised four kids, and ran a day care with 14 kids under the age of four. So I never sat down,” Wilkerson said.
At 72, Wilkerson also battles fibromyalgia and periodic headaches that are so intense, a shot of Demerol is needed to break the pain cycle. But that Demerol injection has been harder to get in recent years.
“I had a headache that lasted four months. Being my age and weaker than normal, I could not get off the couch. I was in agony,” Wilkerson said.
DIVERSIFYING RELIEF OPTIONS
Obah, who has double certification in internal medicine and anesthesia pain management, said his clinic helps patients addicted to opioids with other treatment options and counseling.
“If the patient is willing to work with us, we work with them,” Obah said.
He also vigilantly tracks their progress.
“We do urine testing and check to make sure they’re taking the prescribed medications. That also tells us if they’re doing any street drugs or anything not prescribed by us,” Obah said, adding that his office also routinely checks the state’s controlled substance database to make sure patients aren’t doctor shopping or getting things from other providers that might increase their risk.
“We see patients who want to give up. And we have patients from all walks of life. … All these people need the ability to function and continue to do their work,” Obah said. “We switch things out instead of just increasing dosage.”
Obah’s flexibility and willingness to work with people is appreciated by patients who often have relatives and neighbors who aren’t as understanding.
“I don’t like it when people say ‘You are on drugs,’ ” said Ana Adams, 49, of Layton. “I have battled that stigma, not only with the family but with the community.”
Adams was injured in 2009 when she fell on ice and broke three vertebrae. The injury complicated an existing problem with two disks from an injury two decades earlier. She said she didn’t ask for her chronic pain and she doesn’t appreciate the difficulties she’s experienced because of the actions of addicts.
“I don’t want to have to feel like I am a criminal because I take a medication that relieves the pain and allows me to function,” Adams said. A family member once went through her cupboards, asking if she was adhering strictly to prescribed amounts of her medications.
UTAH’S LEGISLATIVE FIXES
Another of Obah’s patients, Theodore Viegas, 60, of Ogden, said changing rules have made it harder for him to get the medicine he needs to function.
“It’s made my life worse,” he said. “Now, they want to take more away.”
Viegas suffers from many medical problems, including multiple sclerosis, lupus, diabetes and a recently broken heel. But the condition that causes him the most pain stemmed from a series of surgeries on his foot that left him with no cushion between his foot bones and his skin.
Story continues below photo.

SARAH WELLIVER/Standard-Examiner
Theodore Viegas talks about the constant pain he lives with Friday, Nov. 17, 2017, at his sister’s home in Farmington. Viegas keeps a box of more than 32 medications to combat his pain and other symptoms from multiple sclerosis.
He said legislation designed to limit pain medications for addicts isn’t fair for people like him who have a legitimate, chronic need.
Before additional limitations for the drugs in the last few months, Viegas said he was able to do some yard work and “normal things.” Now, he said his days are mostly limited to the couch, even though he has never failed a drug test and never doctor shopped.
“As much as I don’t want to take this medicine, I have to,” he said, pointing to 32 medications he keeps in his safe.
Last March, the Academy of Integrative Pain Management noted a whirlwind of measures Utah lawmakers had just approved that would affect how pain practitioners do their work.
For example, House Bill 50 limits opiate prescriptions for acute conditions to a seven-day supply except in cases where the patient had surgery and their doctor determined that more than a week’s worth was needed. Then a 30-day supply could be prescribed.
And House Bill 90 requires health insurers to establish policies aimed at minimizing the risk of opioid addiction and overdose. Those policies can mirror the 2016 guidelines issued by the Centers for Disease Control and Prevention for using opioids to treat chronic pain. Of the CDC’s 12 recommendations, three principles were seen as key to improving patient care:
- Use nonopioid therapy for chronic pain outside of active cancer, palliative and end-of-life care.
- When opioids are used, prescribe the lowest effective dosage to reduce risks.
- Monitor all opioid patients closely.
From Obah’s perspective, opioids were too often and too liberally prescribed to treat acute pain, which is temporary, such as when someone has sustained an injury or underwent surgery. This overprescribing compounds the problem facing Utah and the nation today. But chronic pain is constant or intermittent with no projected end in sight.
“A lot of the chronic pains arise from not treating acute pain very well, especially surgical pains,” Obah said. “Acute pain, not well treated, can progress into chronic pain where patients need more medications longer. And social isolation and depression can result from chronic pain.”
According to seven months of 2017 data compiled by the Utah Department of Health, between 1.1 and 1.3 percent of all written opioid prescriptions were for a four-to-seven-day supply, while 64.8 to 67 percent were for 30 days or more.
Rep. Ray Ward, a family practitioner from Bountiful, sponsored those two new laws.
“For most short-term things, they should be writing prescriptions for three days” in accordance with CDC guidelines, Ward said. “If you are on narcotics for 10 days in a row, there’s a 10 percent chance of becoming permanently addicted, for 30 days a 30 percent chance of becoming permanently addicted. So you turn a two-week back problem into a lifelong medical problem.”
Ward also believes that prescribing narcotics for first-time chronic pain patients can be counterproductive.
“For someone with chronic arthritis in both knees, they’re thrilled to have the narcotics at first. But three months later they report their pain is back, and if they skip a dose their pain is horrible,” Ward said, referring to the tolerance the body builds to opioids, thus creating the need for increasingly larger doses to achieve the same initial relief.
Prescribing narcotics had been acceptable for decades, Ward added, but getting patients off them is difficult.
“My practice has changed a lot. I now suggest other alternatives,” Ward said. “But patients go elsewhere and start on a long-term narcotic. Every day in my clinic I see the wreckage.”
Obah deals with some of that same wreckage.
“For very severe pain patients … some have been on huge amounts of opioids for up to two decades or more. These patients are now being stigmatized because they’re on opiates. And now their pain providers whom they depend on to maintain their function and quality of life are being forced to turn their backs on them by taking away their meds,” Obah said, empathizing with their pain on several levels. “Some have been dropped by other clinics and resorted to street heroin. So we’re creating a bigger problem than the one we were trying to solve.”
Cindie Dodenbier, a nurse practitioner with several years experience in pain management, works alongside Obah at Lifespring and lamented their lack of opportunity to give input into recent legislation now affecting their patients.
“This clinic is a haven where people can get care and respect,” Dodenbier said. “The travesty here is that we have not been conferred with as a discipline, that these people seem not to matter as valid humans with a very torturous clinical condition. If they could differentiate us out from primary care as the palliative care specialty that we are, it would solve so many problems for so many people.”
Standard-Examiner reporter JaNae Francis contributed to this report.
Contact reporter Cathy McKitrick at 801-625-4214 or cmckitrick@standard.net. Follow her on Twitter at @catmck.